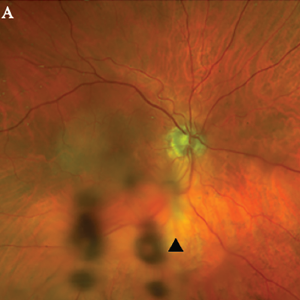
Figure 1A. Optos Fundus photo of the right eye with subtle area of retinal whitening in the macula with mild vitreous opacities inferiorly (arrowhead).
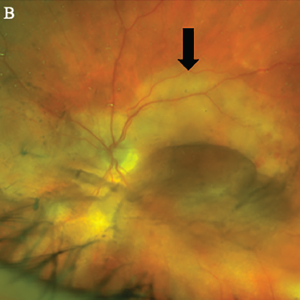
Figure 1B, Optos Fundus photo of the left eye with large placoid area of retinal whitening involving the macula (arrow), with retinal hemorrhages and vitreous opacity temporally.
He denied any eye pain, pain on eye movements, complete vision loss, new neurologic symptoms, fevers, chills, fatigue, weight loss or jaw claudication.
In the clinic, the initial fundoscopic exam appeared normal. Inflammatory markers were significantly elevated with a C-reactive protein (CRP) level of 35.8 mg/L and an erythrocyte sedimentation rate (ESR) of 130 mm/hour.


