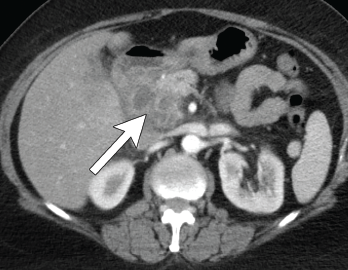
Figure 4. Axial CT showing multilocular abdominal fluid collection.
A 56-year-old woman presented to the hospital with chest and abdominal pain. Her history was notable for pustular psoriasis, psoriatic arthritis (untreated), relapsing-remitting multiple sclerosis (not on therapy), as well as recurrent abscesses over the preceding four years. Abscesses occurred at the chest wall (see Figures 2 & 3, opposite), axilla and pancreas.
She was treated with systemic antibiotics, although aerobic, anaerobic and AFB cultures were repeatedly negative during each of these episodes. Additional testing included negative results for anti-nuclear antibody, anti-neutrophil cytoplasmic antibody, anti-myeloperoxidase antibody, anti-proteinase 3 antibody and human leukocyte antigen B27. Computerized tomography (CT) of the abdomen/pelvis demonstrated a possible duodenal-colonic fistula that was not further evaluated. Her symptoms improved with corticosteroids.
One year later she was admitted with chest and abdominal pain. She was afebrile, hypertensive up to 200/110 mmHg (RR: <120 mmHg systolic, <80 mmHg diastolic), without tachycardia or abnormal respiratory rate. Initial labs were notable for leukocytosis with a total WBC of 22.2 x 109/L (RR: 4.0–11.0 x 109/L) and elevated inflammatory markers with ESR 82 mm/h (RR: 0–30 mm/hour for women over 50) and a CRP of 10.6 mg/dL (RR: 0–0.6 mg/dL). CT scan of the chest/abdomen/pelvis demonstrated a 2.3×4 cm peri-pancreatic abscess with fat stranding and associated lymphadenopathy (see Figures 4 & 5, p. 22).

Figure 5. Coronal CT showing multilocular abdominal fluid collection.
Cultures from the abscess aspirate again failed to identify an organism, and 40 mg of prednisone daily was initiated. Despite this, she developed a new chest wall abscess over the following days. Incision and drainage were performed, with negative cultures. The following day she developed skin erythema, and pain and warmth at the incision and drainage sites. Due to concern for possible cellulitis, corticosteroids were stopped and she was started on antibiotics.


