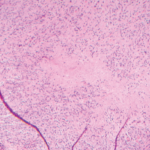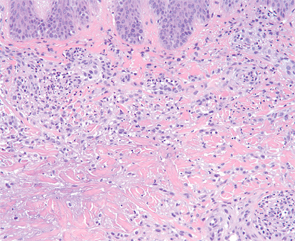
Figure 4: Higher magnification demonstrates aggregates of neutrophils and an interstitial arrangement of histiocytes. (Hematoxylin-eosin stain; original magnification: x400.) Photomicrograph courtesy of Timothy McCalmont, MD.
In patients without a preceding diagnosis of a connective tissue disorder or rheumatoid arthritis, a comprehensive evaluation is warranted and should include serologic testing for antinuclear antibodies, antineutrophil cytoplasmic antibodies (ANCAs), rheumatoid factor (RF) and cyclic citrullinated peptide, as well as a complete blood count with differential and a chest X-ray. In select cases, serum protein electrophoresis and/or immunofixation electrophoresis, viral hepatitis and HIV testing should be considered.2 Even in patients with an established systemic disease, a careful search for an underlying cause is warranted because the development of PNGD may herald the onset of an additional inflammatory or infectious process.
Because PNGD is a rare disorder, evidence for its treatment is anecdotal and limited to case reports and small series. In up to 20% of cases, PNGD resolves without intervention. Therefore, observation alone may be an acceptable management approach.2 In persistent cases, therapy should be directed toward the underlying systemic cause, as optimization of the systemic disorder often improves the skin disease. PNGD-specific treatment may be needed when a systemic association cannot be identified or when the associated condition is under control yet the skin disease persists. In such cases, dapsone, colchicine, and intralesional and systemic corticosteroids are reportedly effective.2,6