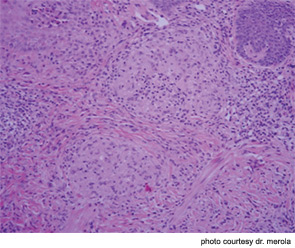
The correct answer is D) Sarcoidosis: This patient’s first presentation of sarcoidosis consisted of skin lesions that were sarcoidal granulomas localized to a single pigment color within her tattoo (note the red pigment areas only are affected). Red tattoo pigment most commonly consists of mercuric sulfide (cinnabar), sienna (ferric hydrate), sandalwood, brazilwood, or organic pigments (aromatic azo compounds). Cutaneous sarcoidosis localized to a tattoo has been well described and several reports demonstrate localization to a single pigment within a given tattoo.
Discussion of Other Choices
- Majocchi’s granuloma occurs when a superficial fungal/tinea infection extends down into hair follicles and creates a deeper inflammatory granulomatous skin infection. This patient did not have superficial scale or other obvious signs of superficial tinea infection. The biopsy did not demonstrate signs of fungal infection and tissue cultures were negative. Topical antifungal agents may be insufficient to treat these infections.
- As discussed above, atypical mycobacterial infection is of particular concern in this patient with a recent tattoo placement. A number of causative mycobacterial strains have been reported, including M. Chelonae, M. Haemophilum, and M. Abscessus.
- A granulomatous hypersensitivity reaction may occur, especially to red color–containing pigment (mercury based). This diagnosis was considered until the patient demonstrated other features of sarcoidosis. The possible diagnosis of sarcoidosis should always be considered in these patients.
- Hypertrophic lichen planus can present as firm, inflammatory nodules over the lower extremities or more diffusely. They may have a characteristic violaceous appearance. While lichenoid reactions to tattoo pigment have been described, this patient’s pathology results rule out this possibility. Atypical forms of lichen planus, in particular mucosal involvement and hypertrophic variants, may be associated with an underlying hepatitis C infection.
Sources:
- Antonovich DD, Callen JP. Development of sarcoidosis in cosmetic tattoos. Arch Dermatol. 2005;141:869-872.
- Rodríguez-Blanco I, Fernández LC, Suárez-Peñaranda JM, Pérez del Molino ML, Esteban J, Almagro M. Mycobacterium chelonae infection associated with tattoos. Acta Derm Venereol. 2011;91:61-62.

Dr. Merola is an instructor in the Department of Dermatology at Harvard Medical School and a fellow in the Rheumatology Division at Brigham and Women’s Hospital, both in Boston. He is the assistant program director for the Combined Medicine-Dermatology training program and a diplomat of the American Board of Dermatology and the American Board of Internal Medicine.