
Figure 3. The patient had flexion contractures of her knees.
months from symptom onset was also found to be associated with improved prognosis. A role for immunosuppressive agents in conjunction with corticosteroids has also been discussed in the literature as possibly improving treatment outcomes.2,6 Methotrexate is often the most commonly used corticosteroid-sparing agent; however, the efficacy of mycophenolate mofetil, azathioprine, tumor necrosis factor inhibitors and other therapies has been detailed in small case series. In one retrospective study of 34 patients, methotrexate used in combination with corticosteroids was needed in 44% of patients due to an unsatisfactory response to corticosteroids alone.6
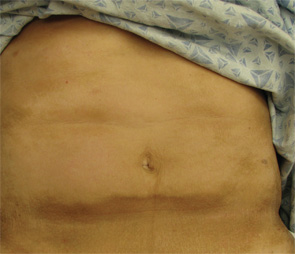
Figure 4. The exam also revealed indurated plaques on the patient’s abdomen.
Because there can be an association with underlying malignancy, most commonly hematologic and myelodysplastic disorders, we advise serum protein electrophoresis and immunofixation testing in all patients. Those patients with cutaneous findings overlying the joints, or those with contractures upon presentation, should receive aggressive physical and/or occupational therapy to prevent morbidity.


