click for large version
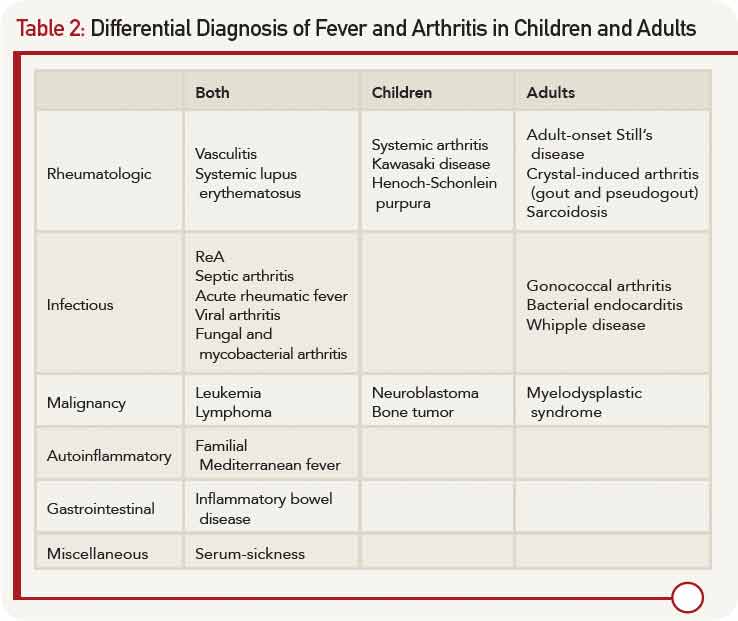
Table 2: Differential Diagnosis of Fever and Arthritis in Children and Adults
Laboratory Results
Laboratory tests confirmed raised markers for inflammation and thrombocytosis. Testing for human leukocyte antigen (HLA) B27, sent from the other hospital, returned positive. Further laboratory workup revealed negative occult fecal blood, and his stool culture was negative for Campylobacter, Enterohemorrhagic E. coli, Salmonella, Shigella, and Yersinia.


