Discussion
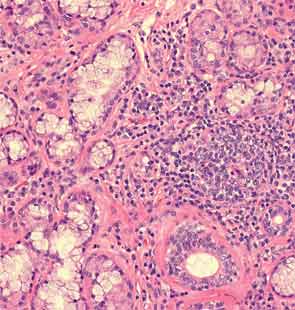
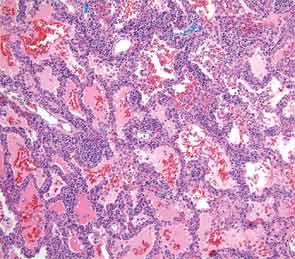
Rheumatologists are often asked to evaluate patients presenting with interstitial lung disease (ILD) in association with a positive ANA or RF, joint, or musculoskeletal symptoms. This case highlights one such typical scenario. The initial concern was for an ANCA-associated disease based on the presence of aural symptoms, hemoptysis, lung disease, and arthritis. However lack of ANCA antibody positivity, absence of any bony erosion on sinus imaging, and subsequent biopsy without histological evidence of vasculitis merited a diagnostic reevaluation.
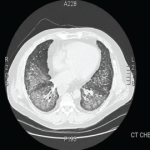
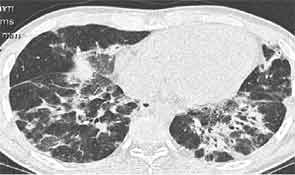
Antisynthetase syndrome is a systemic autoimmune syndrome characterized by a variable combination of ILD, myopathy, fever, joint involvement, and mechanic’s hands with a reported prevalence of 1.5 per 100,000. Its hallmark is the presence of antibodies directed against aminoacyl-transfer RNA synthetase of which the most frequent is the anti-Jo-1 antibody that accounts for about 80% of all cases of antisynthetase syndrome.1 Other relatively common antibodies include anti-PL-7 and anti-EJ.2 Anti-Jo-1 antibodies are present in about 30% of patients presenting with myositis and it is in the setting of myositis that these antibodies are usually tested to diagnose antisynthetase syndrome. ILD, however, is the most frequently occurring manifestation of antisynthetase syndrome and is reported in 75% to 89% of all cases.3 Lung involvement is the most important determinant of prognosis.