Image Credit: Molodec/shutterstock.com
Case report: A 78-year-old Caucasian female presented to our outpatient rheumatology clinic with pain in her bilateral shoulders, hands and knees that began suddenly one month earlier. She admitted to stiffness in her hands lasting several hours, and expressed an inability to extend her fingers. She denied fever, rashes, jaw claudication, headache or visual changes. She also denied having night sweats, unintentional weight loss, shortness of breath or abdominal pain.
Her past medical history was unremarkable, with no prior history of malignancy. She did not take any medication. Her vital signs were stable, and she was afebrile. She had normal breath sounds and a regular heart rate and rhythm. She exhibited no abdominal tenderness.


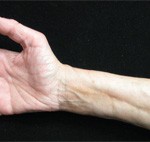
Figure 1A (left) & Figure 1B: These images show the patient’s hands on initial presentation to the rheumatologist, with visible flexion contractures of all digits and swelling, erythema and pain on palpation.

Dr. Kesselman
A diagnosis of palmar fasciitis and polyarthritis syndrome (PFPAS) was rendered. The patient was started on 20 mg prednisone daily with a slow taper planned, and she was advised to follow up with her primary care physician for cancer screening. She had a DEXA scan performed, which showed a normal bone density, with a lumbar spine T score of –0.7, and a hip T score of –0.9. She refused treatment for prevention of glucocorticoid-induced osteoporosis, but agreed to take daily calcium and Vitamin D.