The pathology of the resected portion showed a small transmural defect with acute serositis, consistent with perforation. Multiple ulcers were identified in the specimen.
The patient’s skin and respiratory status improved, and he was weaned off the mechanical ventilation. His renal function returned to normal. His course was complicated by the GI manifestations of his disease. Following the bowel surgery, he continued to show improvement; he was placed on tube feedings and started on an oral diet. His GI bleeding resolved completely, and he did not require further transfusions.
Discussion
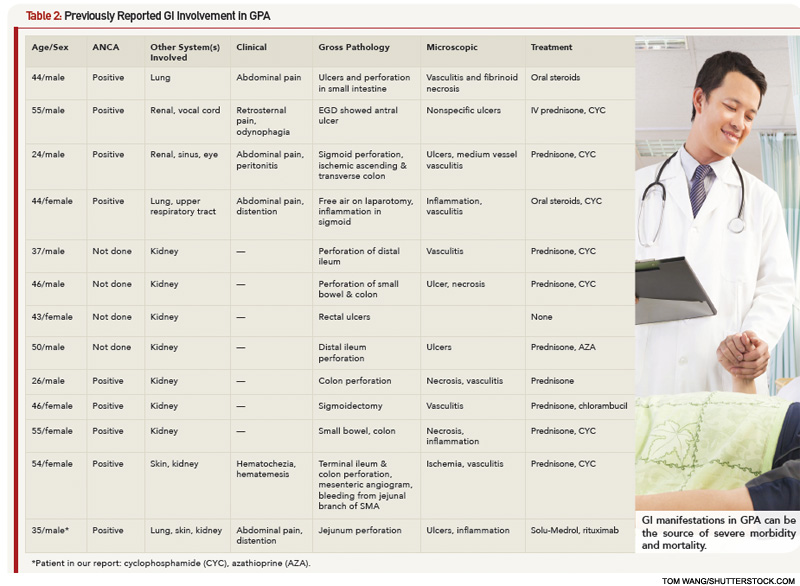
GPA affecting the GI tract has been infrequently reported in literature. There are case reports of the disease affecting parts of the digestive tract: esophagus, stomach, small intestine or colon.3 Esophagogastroscopy may reveal multiple superficial small ulcerations or small (0.5 to 1 cm) polyps in the esophagus, the stomach or the pylorus. Vasculitis mainly affects the distal small bowel or colon.


