Discussion
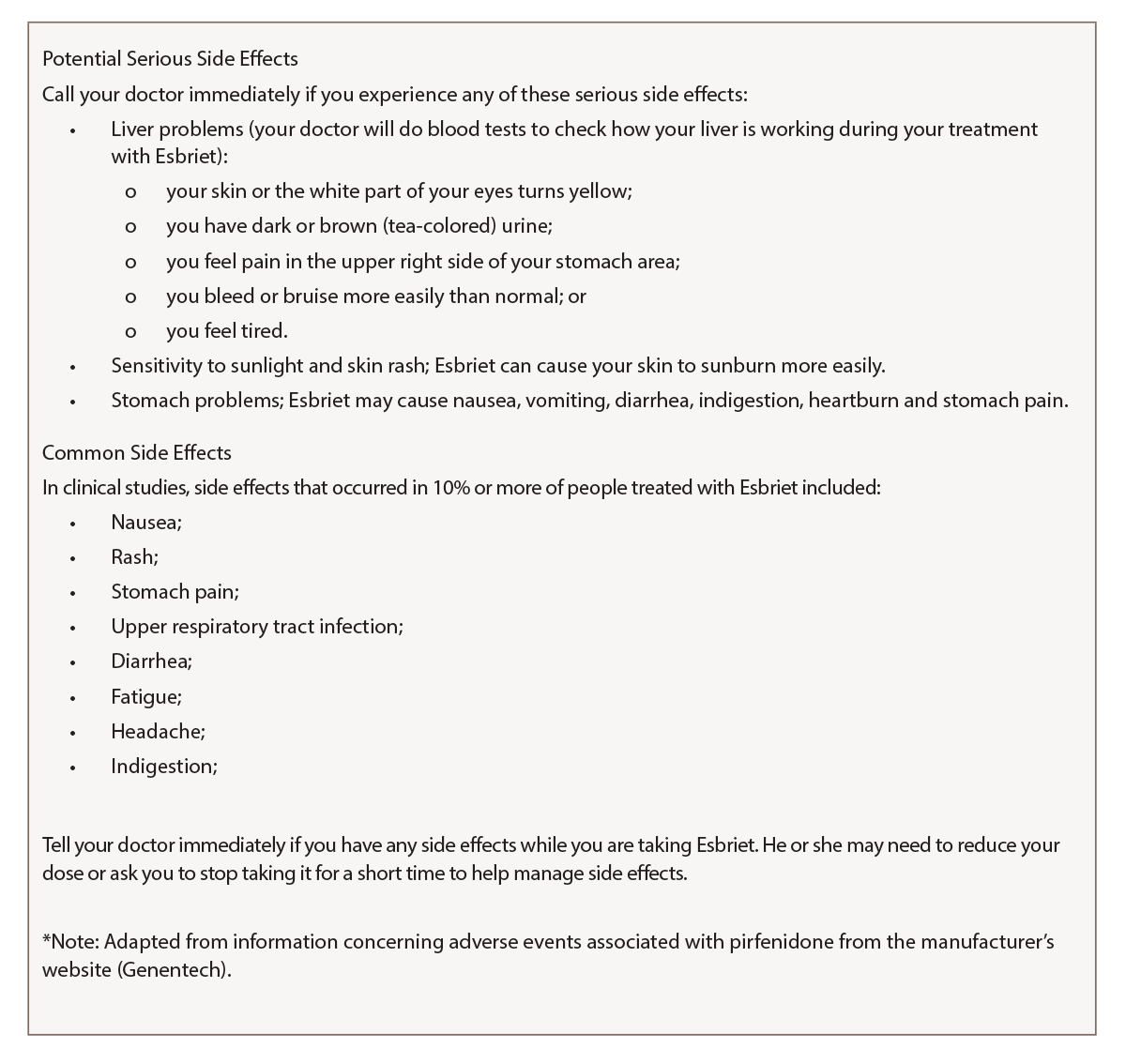
(click for larger image) Figure 3: Side Effects of Esbriet (Pirfenidone)*
In this report, we present three new applications of the MDHAQ. First, RAPID3 documented substantial improvement over six months in a patient with a non-rheumatic disease, pulmonary fibrosis, based on usual routine MDHAQ completion in the clinic waiting area. RAPID3 may be useful in many non-rheumatic diseases. All ambulatory individuals wish to be as functional and pain free as possible and experience overall well-being, reflecting the three RAPID3 components, which are identical to the RA core data set.
Second, a remote electronic MDHAQ documented adverse events to a medication, pirfenidone, as substantially elevated RAPID3 and fatigue VNS scores, and seven new specific symptoms (see Figure 2, opposite) which were listed as adverse events for pirfenidone (see Figure 3, above right). A face-to-face visit did not appear mandatory, because he reported an unchanged pulmonary situation and virtually all new symptoms could be attributed to the pirfenidone (and possible withdrawal from low-dose prednisone and methotrexate). Discontinuation of pirfenidone, reinstatement of 10 mg prednisone, contact if symptoms were worsening and remote electronic MDHAQ review two days later appeared reasonable to avoid further acute stress to an elderly patient who required continuous oxygen therapy. Clear improvement two and five days later were documented on the remote electronic MDHAQ symptom checklist, which would not have been available if only RAPID3 were queried.
