Dr. Bose notes that the diagnosis is primarily clinical, but that “advanced imaging like magnetic resonance imaging (MRI) or ultrasound can help distinguish whether there are changes of inflammatory arthritis or if the presentation is purely mechanical.”
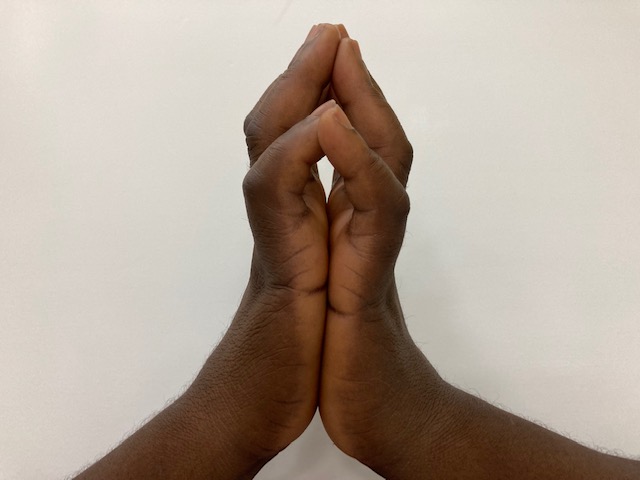
FIGURE 1: The Prayer Sign of Limited Joint Mobility or Diabetic Cheiroarthropathy. A 53 year old woman with a history of type 2 diabetes mellitus of 31 years with associated microvascular complications presented with a 1 year history of gradually worsening, stiffness of the fingers. She reported occasional hand pain with use and impairment of fine movement. Thickened, tight and waxy skin was noted along with fixed flexion contractures of the interphalangeal joints with impaired grip strength and she demonstrated the prayer sign. Strict blood glucose control measures were implemented and physical therapy was recommended.
On clinical examination, patients will be unable to flatten their palms together, known as a positive prayer sign (see Figure 1), or similarly will be unable to place their hand flat on a table.


