‘We don’t often think about diabetes as a rheumatic disease,” says Dr. Bharat Kumar, “but it has a lot of musculoskeletal and immunologic manifestations. Recognizing these manifestations can help rheumatologists better manage their patients and direct therapy.’

 Diabetes itself can present with an array of non-inflammatory rheumatic manifestations that may mimic inflammatory diseases, such as rheumatoid arthritis, scleroderma and myositis. Rheumatic manifestations of diabetes can lead to functional limitations that impede exercise and further compromise glycemic control, although they are often overshadowed by the more familiar complications of microvascular disease, such as neuropathy, retinopathy and nephropathy.2 Indeed, the musculoskeletal manifestations of diabetes are not mentioned in the practice guidelines from the American Diabetes Association.3,4
Diabetes itself can present with an array of non-inflammatory rheumatic manifestations that may mimic inflammatory diseases, such as rheumatoid arthritis, scleroderma and myositis. Rheumatic manifestations of diabetes can lead to functional limitations that impede exercise and further compromise glycemic control, although they are often overshadowed by the more familiar complications of microvascular disease, such as neuropathy, retinopathy and nephropathy.2 Indeed, the musculoskeletal manifestations of diabetes are not mentioned in the practice guidelines from the American Diabetes Association.3,4
In this review, we explore the lesser known rheumatic entities of diabetes, such as diabetic cheiroarthropathy, scleredema and diabetic myonecrosis, with clinical pearls and insights provided by experts in the field. We also highlight the common musculoskeletal diseases with increased incidence in patients with diabetes, such as carpal tunnel syndrome, Dupuytren’s contracture and stenosing tenosynovitis. For each entity, we discuss the presenting signs and symptoms, diagnosis and management.
Diabetic Cheiroarthropathy
Diabetic cheiroarthropathy has many different illustrative names, including the syndrome of limited joint mobility, diabetic contractures, stiff hand syndrome and diabetic stiff hand. It is characterized by a progressive resistance to passive and active range of motion, often beginning in the hands, and seen in patients with diabetes.

Dr. Bose
Nilanjana Bose, MD, a rheumatologist in private practice at Lonestar Rheumatology, Houston, and an adjunct professor with the University of Texas Medical Branch at Galveston, notes, “Although [diabetic cheiroarthropathy] isn’t seen routinely, it is a diagnosis that you have to keep in your differential for joint stiffness.”
Importantly, it is a painless entity, and patients will present with “contractures and fibrosis with waxy skin on the hands. Distinguishing it from rheumatoid arthritis should be fairly straight forward for the rheumatologist,” says Dr. Bose. It can also be distinguished from Dupuytren’s contracture given the absence of thickening or nodularity of the palmar fascia.5
The reported prevalence of diabetic cheiroarthropathy varies widely, from 8–53%, depending on the definition used and population studied.5 Diabetic cheiroarthropathy is associated with the duration and severity of diabetes, but can be seen in prediabetes and can be out of proportion to the A1C.5,6
Patients may describe a loss of grip strength, inability to perform fine motor movements and generally impaired hand function. They may also have dysesthesia due to concomitant diabetic polyneuropathy. Contractures mostly occur in the proximal interphalangeal and metacarpophalangeal joints, and tend to progress over time from the fourth and fifth digits radially toward the second and third digits.5
Dr. Bose notes that the diagnosis is primarily clinical, but that “advanced imaging like magnetic resonance imaging (MRI) or ultrasound can help distinguish whether there are changes of inflammatory arthritis or if the presentation is purely mechanical.”
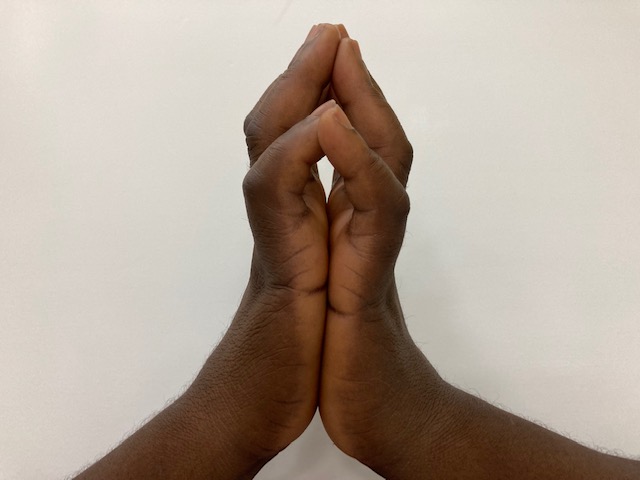
FIGURE 1: The Prayer Sign of Limited Joint Mobility or Diabetic Cheiroarthropathy. A 53 year old woman with a history of type 2 diabetes mellitus of 31 years with associated microvascular complications presented with a 1 year history of gradually worsening, stiffness of the fingers. She reported occasional hand pain with use and impairment of fine movement. Thickened, tight and waxy skin was noted along with fixed flexion contractures of the interphalangeal joints with impaired grip strength and she demonstrated the prayer sign. Strict blood glucose control measures were implemented and physical therapy was recommended.
On clinical examination, patients will be unable to flatten their palms together, known as a positive prayer sign (see Figure 1), or similarly will be unable to place their hand flat on a table.
Unfortunately, there are few therapeutic options for diabetic cheiroarthropathy. Dr. Bose says, “Our limited option is educating the patient on improving diabetic control,” although, it isn’t clear whether improved glycemic control will contribute to meaningful improvements in joint mobility.7
In Dr. Bose’s experience, “flexibility is often quite restricted by the time they present with musculoskeletal manifestations.” Physical and occupational therapy can be tried to improve mobility, but may be of limited benefit.8
“I might see these patients for a few visits to make sure that we aren’t missing something concurrently,” says Dr. Bose. “It can be hard to know right off the bat with mimics, and things can evolve with time. While rheumatoid arthritis and diabetic cheiroarthropathy in the same patient would be rare, it could happen, so one should follow the patient for a year or two to see how they progress.”
Diabetic cheiroarthropathy can be associated with a digital sclerodactyly that looks similar to scleroderma, and thus is sometimes called pseudoscleroderma. Notably, Raynaud’s phenomenon will be absent and nailfold capillaries will be normal. Digital ulcerations of the hands will also be absent. When present, digital ulcerations should trigger evaluation for connective tissue disease.
Scleredema
Scleredema is a dermatologic condition characterized by excess collagen deposition in the skin, and has three distinct subtypes. Type I, also known as scleredema adultorum of Buschke, is often self-limited and associated with a preceding viral illness. Type II is associated with paraproteinemia and risk of myeloma, and type III, the focus of this section, is an indolent form known as scleredema diabeticorum, associated with difficult-to-control diabetes.6
In diabetes, hyperglycemia leads to on-enzymatic glycosylation of collagen that becomes resistant to breakdown, leading to an accumulation of abnormal collagen in the skin, which is doughy and indurated, rather than tight and shiny as seen in scleroderma.6,8

Dr. Schiopu
Dr. Elena Schiopu, professor of medicine at the Medical College of Georgia, Augusta, with clinical and research expertise in scleroderma and myositis, often encourages her trainees to examine patients for scleredema in its usual “cape-like distribution,” looking for symmetric skin thickening along the neck, upper back and shoulders. In severe cases, the face can also be involved.
Several important features distinguish scleredema from scleroderma. Namely, scleredema spares the hands and feet, Raynaud’s will be absent, and nailfold capillaries will be normal. Systemic organ involvement is rare, but the heart, lungs and tongue can be affected. Dr. Schiopu says “pigmentary changes, which we would expect to see in scleroderma, would also be absent.”
Dr. Schiopu notes that she is often “impressed with how much scleredema can impair quality of life, with movements like showering—even breathing—impaired,” given involvement of the upper back and chest wall.
Diagnosis of scleredema is clinical, but Dr. Schiopu prefers skin biopsy to exclude other etiologies. It is also important to specifically query type II scleredema with serum protein electrophoresis (SPEP) and immunofixation, given the risk of underlying monoclonal gammopathy or myeloma.
Management of scleredema is challenging because various therapies, such as ultraviolet light, intralesional steroids, radiation and immunosuppression, have limited benefit.8 Dr. Schiopu explains that “the disease-modifying role here isn’t as visible. I haven’t found any immunosuppressive agents with any signal, including intravenous immunoglobulin. Additionally, diabetes itself is a comorbidity that already complicates the decision to add immunosuppression. The best option we have is tight control of diabetes.”
Diabetic Myonecrosis
Diabetic myonecrosis is also known as diabetic muscle infarction, spontaneous aseptic diabetic muscle infarction and ischemic myonecrosis.8 It is an under-recognized complication of diabetes, with fewer than 200 cases reported in the literature.10 Dr. Schiopu notes that “although [diabetic myonecrosis] is rare, it is important to keep in mind.”
Patients present with acute-onset, painful swelling of an affected muscle. The thigh is most commonly involved, and a palpable mass may be present.9 Myonecrosis is distinct from diabetic amyotrophy (i.e., Bruns-Garland syndrome), in which there is muscle wasting, weakness and pain due to diabetic neuropathy, such as at the lumbosacral plexus.
“Diabetic myonecrosis should always be listed in the differential, especially if a patient has very localized, exquisitely painful swelling and poorly controlled diabetes,” says Dr. Schiopu.
Myonecrosis may be confused with idiopathic inflammatory myopathy (IIM), given the presence of fever in 10% of patients, elevated erythrocyte sedimentation rate in over 50%, creatine kinase (CK) elevations and indistinguishable changes of muscle edema on MRI.9
Sureja et al. described a case of a 59-year-old man who presented with insidious pain in both thighs, resulting in immobility and mimicking IIM.11 MRI showed symmetrical involvement of the thigh muscles with hyperintensities on short-tau inversion recovery imaging, and a CK of approximately 300 U/L. The patient had a similar prior episode and muscle biopsy that showed ischemic necrosis of muscle fibers. Thus, a diagnosis of recurrent diabetic myonecrosis was made. The patient ultimately improved with supportive management over several weeks.
Key distinguishing features from IIM are that diabetic myonecrosis tends to be acute in onset, with only mild elevations in CK, and it is often unilateral, sparing the upper extremities.9 Autoantibodies should be negative, and there will be no additional signs or symptoms of connective tissue disease, such as interstitial lung disease, inflammatory arthritis or cutaneous disease. Dr. Schiopu has found overlying erythema of the affected muscle can occur and may be confused with cellulitis.
Treatment of diabetic necrosis is “very much supportive,” says Dr. Schiopu. Like other musculoskeletal manifestations, it is unclear whether strict diabetes control will have a meaningful impact on prevention, but it is one of few options. Patients will likely need short-term pain control and should engage with physical therapy for muscle strengthening.9
Additional Musculoskeletal Findings in Diabetes
Carpal tunnel syndrome
Carpal tunnel syndrome is an entrapment neuropathy due to compression of the median nerve as it courses through the carpal tunnel. Patients may present with numbness and tingling in the thumb, index and middle finger, and sometimes weakness with thumb abduction.
Diabetes is a known risk factor for carpal tunnel syndrome because diabetes induces structural changes in the connective tissues of tendons surrounding the median nerve, leading to nerve compression.12 Patients with diabetes have 90% higher odds of developing carpal tunnel syndrome and are more likely to have it in both wrists.13 In a cross-sectional study of 100 patients with diabetes, approximately 20% had carpal tunnel syndrome.14
Diagnosis and management of carpal tunnel syndrome is the same in patients with and without diabetes, although surgical release is more common in patients with diabetes.15 Carpal tunnel syndrome can coexist with diabetic polyneuropathy, thus it is important to establish whether peripheral nerve symptoms are secondary to nerve entrapment or diabetic polyneuropathy because patients with neuropathy may not sustain the same improvement after carpal tunnel release as those without polyneuropathy.16
Dupuytren’s contracture
Patients with Dupuytren’s contracture present with thickened, fibrotic nodules and cords within the palmar fascia leading to digital contractures, most commonly at the fourth and fifth digits.17 Dupuytren’s must be distinguished from diabetic cheiroarthropathy, which does not present with fibrotic nodules or cords, and tends to affect all digits but the thumb. Notably, the two can co-occur.
Dupuytren’s in patients with diabetes has been shown to occur four times more frequently than in those without it, and its prevalence is related to age and duration of diabetes.18
Diagnosis of Dupuytren’s is clinical. Patients who develop flexion contractures can undergo surgery (i.e., open fasciectomy), percutaneous needle aponeurotomy or collagenase injection. Surgery has been shown to have higher success rates at longer term follow-up.19
Stenosing flexor tenosynovitis
Stenosing flexor tenosynovitis, also known as trigger finger, is characterized by localized inflammation of the flexor tendon sheath, rather than the tenosynovium (as its name would suggest), leading to finger locking with failure of active extension. Patients may describe a painful popping or clicking sound when the digit is extended. With time, disuse of the digit can lead to secondary proximal interphalangeal contractures.20 The ring finger is most commonly affected, but multiple digits may be involved, and it can be bilateral.21
Trigger finger is more common in women, and estimated to occur at 5–11% in patients with diabetes, vs. 2–3% in the general population.22 The incidence in patients with diabetes is related to duration of diabetes, but not degree of diabetic control.18
First-line therapy includes splinting and corticosteroid injection, although the latter may be less successful in patients with diabetes, and success rates decline with every repeat injection.5,20 Surgical release is indicated if injection should fail.
Conclusion
The intersection of diabetes mellitus and rheumatic diseases presents a unique set of challenges for both diagnosis and management. The non-inflammatory rheumatic manifestations of diabetes, including diabetic cheiroarthropathy, scleredema and diabetic myonecrosis, can mimic rheumatic conditions and lead to significant functional impairment. Awareness and understanding of these manifestations are crucial for accurate diagnosis and to avoid unnecessary immunosuppression.
Likewise, carpal tunnel syndrome, Dupuytren’s contracture and trigger finger are common among patients with diabetes. By recognizing and addressing these musculoskeletal complications, providers can enhance the overall quality of life for patients with diabetes.
Michael J. Cammarata, MD, is an assistant professor of medicine at the Johns Hopkins School of Medicine, Baltimore.
References
- National Diabetes Statistics Report. Centers for Disease Control and Prevention. 2024 May 15. https://www.cdc.gov/diabetes/php/dataresearch/index.html.
- Hill NE, Roscoe D, Stacey MJ, Chew S. Cheiroarthropathy and tendinopathy in diabetes. Diabet Med. 2019 Aug;36(8):939–947.
- Larkin ME, Barnie A, Braffett BH, et al. Musculoskeletal complications in type 1 diabetes. Diabetes Care. 2014 Jul; 37(7):1863–1869.
- American Diabetes Association Professional Practice Committee. Comprehensive medical evaluation and assessment of comorbidities: Standards of care in diabetes–2024. Diabetes Care. 2024 Jan;47(Suppl1):S52–S76.
- Kapoor A, Sibbitt WL Jr. Contractures in diabetes mellitus: The syndrome of limited joint mobility. Semin Arthritis Rheum. 1989 Feb; 18(3):168–180.
- Nashel J, Steen V. Scleroderma mimics. Curr Rheumatol Rep. 2012;14(1):39–46.
- Lieberman LS, Rosenbloom AL, Riley WJ, et al. Reduced skin thickness with pump administration of insulin. N Engl J Med. 1980 Oct;303(16):940–941.
- Morgan ND, Hummers LK. Scleroderma mimickers. Curr Treatm Opt Rheumatol. 2016 Mar;2(1):69–84.
- Trujillo-Santos AJ. Diabetic muscle infarction: An underdiagnosed complication of longstanding diabetes. Diabetes Care. 2003 Jan; 26(1):211–215.
- Horton WB, Taylor JS, Ragland TJ, et al. Diabetic muscle infarction: A systematic review. BMJ Open Diabetes Res Care. 2015 Apr;3(1):e000082.
- Sureja NP, Devarasetti PK, Rajasekhar L. Diabetic myonecrosis: An unusual mimicker of idiopathic inflammatory myositis. J R Coll Physicians Edinb. 2020 Jun;50(2):148–151.
- Burner TW, Rosenthal AK. Diabetes and rheumatic diseases. Curr Opin Rheumatol. 2009 Jan;21(1):50–54.
- Sanjari E, Raeisi Shahraki H, G Khachatryan L, et al. Investigating the association between diabetes and carpal tunnel syndrome: A systematic review and meta-analysis approach. PLoS One. 2024 Apr;19(4):e0299442.
- Gamstedt A, Holm-Glad J, Ohlson CG, et al. Hand abnormalities are strongly associated with the duration of diabetes mellitus. J Intern Med. 1993 Aug;234(2):189–193.
- Monjed A. Diabetes and Rheumatology. In: Skills in Rheumatology. Singapore: Springer;2021. https://www.ncbi.nlm.nih.gov/books/NBK585735.
- Zimmerman M, Dahlin E, Thomsen NOB, et al. Outcome after carpal tunnel release: Impact of factors related to metabolic syndrome. J Plast Surg Hand Surg. 2017 Jun;51(3):165–171.
- Knoedler TG, Gaertner AP, Wilkinson PJ, et al. Incidence, prevalence, and outcomes of hand manifestations in patients with diabetes mellitus: A comprehensive literature review. Hand (N Y). 2024 Jan 30;15589447231219522.
- Chammas M, Bousquet P, Renard E, et al. Dupuytren’s disease, carpal tunnel syndrome, trigger finger, and diabetes mellitus. J Hand Surg Am. 1995 Jan;20(1):109–114.
- Räisänen MP, Leppänen OV, Soikkeli J, et al. Surgery, needle fasciotomy, or collagenase injection for dupuytren contracture: A randomized controlled trial. Ann Intern Med. 2024 Mar;177(3):280–290.
- Makkouk AH, Oetgen ME, Swigart CR, et al. Trigger finger: Etiology, evaluation, and treatment. Curr Rev Musculoskelet Med. 2008 Jun;1(2):92–96.
- Moore JS. Flexor tendon entrapment of the digits (trigger finger and trigger thumb). J Occup Environ Med. 2000 May;42(5):526–545.
- Csonka V, Varjú C, Lendvay M. Diabetes mellitus-related musculoskeletal disorders: Unveiling the cluster of diseases. Prim Care Diabetes. 2023 Dec;17(6):548–553.


