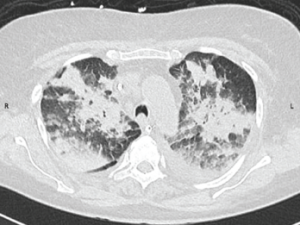
Figure 1: CT Scan of the Chest
A CT scan of the chest obtained without intravenous contrast demonstrates diffuse patchy and groundglass opacifications with upper lobe predominance. These findings are consistent with pulmonary hemorrhage. In addition, bilateral pleural effusions are seen.
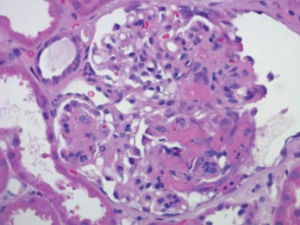
Figure 2: Renal Biopsy
Biopsy specimen of the kidney stained with hematoxylin and eosin demonstrates a necrotizing glomerulonephritis with a fibrinous crescent within the glomerulus. Immune-complex deposits were not seen on electron microscopy (image not shown).
Case Report
A 78-year-old Caucasian woman presented to an outside hospital with a one-week history of shortness of breath and diffuse joint pains in her bilateral knees and shoulders. Her medical history included hypertension not controlled by any medications, an appendectomy, multiple family members with rheumatoid arthritis and a five pack-year smoking history. She did not take any medications at home. Three weeks prior to presentation, she underwent a tooth extraction for a dental abscess and was given a course of penicillin.

