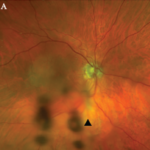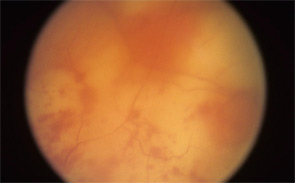
figure 1: Acute retinal necrosis from herpes virus infection.
The rheumatologic perspective was important in this case because we know that patients with a systemic vasculitis, such as polyarteritis or Wegener’s granulomatosis, rarely develop retinal vasculitis from the disease itself—especially if adequately treated. The ophthalmology perspective was equally important because the diagnosis of ARN is usually made by clinical examination that requires indirect ophthalmoscopy to identify the characteristic lesions. These lesions are often in the peripheral retina. Polymerase chain reaction (PCR) tests for a specific virus using surgically obtained ocular fluid can confirm the diagnosis. By amalgamating expertise in rheumatology and ophthalmology, we were able to appropriately diagnose this patient. The proper treatment of ARN is to reduce immunosuppression and initiate anti-viral therapy.
Ophthalmology Refresher
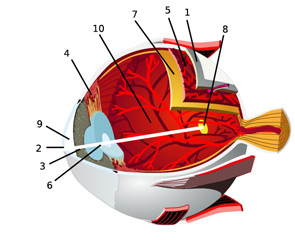
In an effort to facilitate communications with our ophthalmologic peers, this article will review the anatomy of the eye and the salient types of involvement in major rheumatologic diseases. (See Figure 2, for an overview of ocular anatomy.)