X-rays of his left shoulder revealed mild periosteal elevation and hyperostosis of the proximal humerus and distal acromion, and the radiograph of his right knee revealed a subtle osteolytic, erosive lesion on the lateral side of the femur near the joint margin. Magnetic resonance imaging (MRI) of the cervical, thoracic and lumbar spine revealed multifocal, enhancing lesions consistent with marrow edema (see Figures 2A and 2B, below). The brain MRI did not reveal any intracranial lesions, but clearly revealed the cutaneous abscesses on his scalp (see Figure 2C).
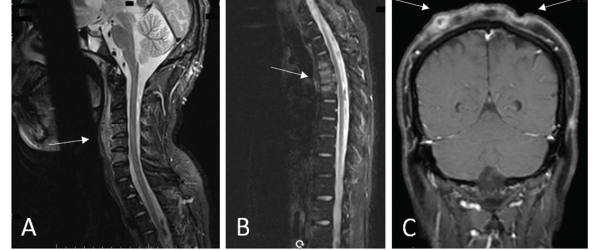
Figures 2a, b, c
(A) An MRI of the cervical spine revealed multilevel, anterior-predominant, marrow edema extending from C3–C7 with paravertebral edema anteriorly (see white arrow). (B) An MRI of the thoracic spine revealed marrow edema of T3–T5 with mild anterior, superior corner erosion of T5 (see white arrow). (C) An MRI of the brain revealed no intracranial lesions, but note the obvious cellulitis and abscess formation on the scalp (see white arrows).
A biopsy of the T4 vertebral body revealed no evidence of bacterial, acid-fast bacilli, fungal or mycobacterial infection. Surgical pathology of the T4 vertebra revealed only hypercellular marrow tissue without evidence of malignancy.

