On presentation, she was afebrile and non-tachycardic. Blood cultures were negative. A physical exam revealed full range of motion in both hips, but was notable for tenderness with internal and external rotation of the left hip. No other joint swelling was noted.
Her hemoglobin at baseline was 9.1 g/dL. Her white blood cell count was 5.7 B/L and remained within normal limits. Her erythrocyte sedimentation rate (ESR) was 30 mm/hour, and C-reactive protein (CRP) was 0.82 mg/dL. Parathyroid hormone intact was elevated at 2,305 pg/dL, calcium was 9.54.6 mg/dL, and phosphorous was elevated at 4.6 mg/dL. Alkaline phosphatase was elevated at 286 units/L.
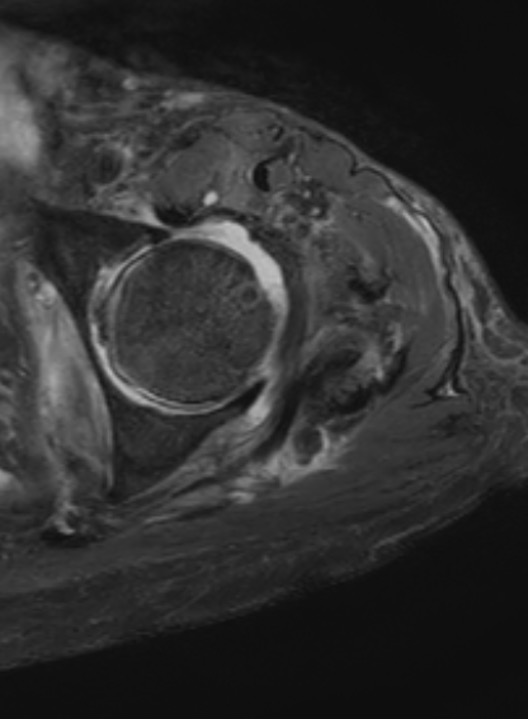
FIGURE 1: T2-weighted axial MRI of the hip with contrast showing periarticular erosion and left hip joint effusion. (Click to enlarge.)
An X-ray of her left hip revealed loss of the subchondral bone along the acetabulum concerning for a septic joint. She then had a computerized tomography (CT) scan of the hip that showed background changes of renal osteodystrophy involving the osseous structures of the bilateral sacroiliac joints and bilateral hip articulations, with findings concerning for superimposed left hip joint septic arthritis. A magnetic resonance imaging (MRI) scan revealed a large joint effusion, periarticular erosion and synovitis, as well as edema involving the left periarticular musculature, most pronounced in the adductor compartment (see Figure 1).
