At the three-month follow-up visit, a more detailed evaluation of her ANCA profile by Western blot analysis revealed variable reactivity to neutrophil elastase (NE) and cathepsin G (CG) in addition to PR3 (see Figure 3). At her 12-month clinic visit, the patient stated that she had completely abstained from any cocaine use and noticed no new skin eruptions. Her old skin lesions have healed with significant scarring. She is treated with HCQ 400 mg daily for her lupus symptoms consisting of intermittent arthritis flares.
Patient 2
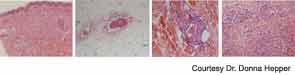
A 54-year-old white female with history of recurrent methicillin-resistant Staphylococcus aureus (MRSA) abscesses presented to the emergency department with a history of painful skin rash, fatigue, and migratory polyarthralgias involving small joints of the hands, knees, and ankles. She worked as an exotic dancer and admitted to inhalational use of marijuana and cocaine regularly. She denied intravenous drug use. Physical exam was significant for purpuric, erythematous nonblanching macules, and patches over the flexor and extensor surface of her legs, buttocks, bilateral breasts, and left pinna, including the lobe and left cheek (see Figure 4. Necrotic skin overlying these areas along with hemorrhagic bullae was noted. A workup for endocarditis was negative. The urine drug screen was positive for cocaine. Serologic testing was significant for positive ANCA 1:320 that reacted with MPO 27, PR3 11, ESR 37 mm/hr, and CRP 82 U. The infectious screen, ANA, anti-dsDNA, extractable nuclear antigen, cryoglobulins, ACL, RF, anti-CCP antibodies were all negative, and complement levels were normal. Skin biopsy findings are shown in Figure 2 and summarized in Table 1 . They revealed vasculopathic dermatitis with intravascular thrombi, dermal abscess formation over the cheek, and leukocytoclastic vasculitis with vascular complement reactivity to type IV collagen. A presumptive diagnosis of cocaine-/levamisole-associated vasculitis was made. The patient was counseled to abstain from further illicit drug use. A two-week course of oral prednisone 20 mg daily was prescribed with dramatic improvement of her skin rash, which healed with scarring.
