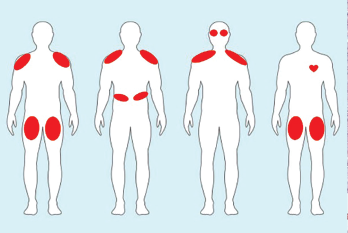
Figure 2. Examples of ICI-myositis muscle involvement. From left: 1) Symmetric, proximal large muscle involvement. 2) Proximal upper arm with diaphragmatic involvement leading to respiratory distress. 3) Proximal upper arm with neck weakness and ocular muscle ptosis resembling myasthenia gravis. 4) Bilateral thigh involvement with myocarditis.
In the case presented, the key first step in management is prompt recognition of the problem and its potential for severe morbidity and mortality, including concomitant myocarditis. This patient should be hospitalized and managed by a multidisciplinary team that optimally includes a neurologist and a rheumatologist, as well as a cardiologist if troponin levels are elevated.
CK and troponin should be tracked over time, even if the patient has no cardiac complaints on initial presentation. An electrocardiogram and an echocardiogram should also be performed. In patients with suspected myocarditis, cardiac MRI and endomyocardial biopsy are often performed.



