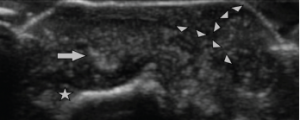
Figure 4: Ultrasound Image of the Bullous Lesion
Dorsal transverse view of the right second DIP. Note the “wet sugar clump” appearance (arrowheads) of the tophaceous material extending to the outer layer of the lesion. Extensor tendon (arrow) is seen overlying the distal phalanx (star).
Hyperuricemia, defined as the point at which serum uric acid levels exceed the threshold for saturation of approximately 6.8 mg/dL, will result in crystalline deposition of monosodium urate within tissues.2 Monosodium urate (MSU) crystals are responsible for starting the inflammatory cascade that is the hallmark of an acute gout attack. MSU deposition, destabilization and reabsorption within joints stimulates release of IL-1β from mononuclear phagocytes though activation of the NLRP3 inflammasome, resulting in local and systemic inflammatory changes, as well as a dramatic local hypernocioception.2 The classic inflammatory arthritis is associated with infiltration of neutrophils into the synovial membrane in response to the inflammatory cascade that follows.2
Chronic hyperuricemic states result in the formation of tophi, dense MSU deposits that often form in joints and also in subcutaneous tissues.3 Due to the crystalline nature of the disease, it’s tempting to consider these as biologically inert lesions outside dramatic inflammatory episodes. But the chronic inflammatory response to MSU deposition consists of granulomatous formations of CD68+ macrophages encasing the crystalline MSU core described by Dalbeth et al, with a fibrovascular zone containing plasma cells and few CD8+T cells and CD20+ B cells surrounding the middle layer, or corona, of macrophages and scattered osteoclasts.
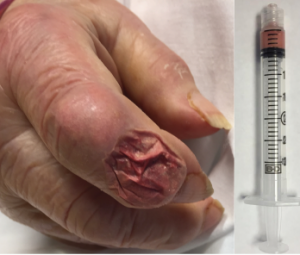
Figure 5: Aspirate of the Bullous Lesion
A thick, chalky aspirate was withdrawn from within the bullous lesion, with granular material having the consistency of wet sand in a serosanguinous suspension.
IL-1β is highly expressed in the corona of macrophages in tophi, which appear to be inversely related to the chronicity of the lesion.3 TGFβ is also simultaneously expressed by macrophages in the same lesion, supporting the chronic inflammatory balance that is being regulated locally by macrophages involved in the granulomatous sequestering of MSU crystal deposits to form tophi. What the chronic tophaceous lesion lacks is the profound neutrophil response, which characterizes an acute gouty attack. However, the expression of IL-1β in the seemingly latent phase demonstrates the chronic inflammatory nature of MSU deposition from the hyperuricemic state.3
Cutaneous manifestations of hyperuricemia have classically been described as variations of tophus formation, with dense conglomerations of MSU depositing in the skin. Within the cutaneous spectrum of disease caused by increased urate burden, a wide range of chronic tophaceous lesions have been described, from isolated large, bulky tophus formation to a miliary appearance of scattered, small tophus formation.
