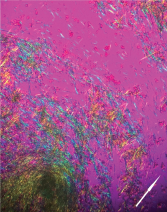
Figure 6: Polarized Microscopy of the Aspirate
Negatively birefringent monosodium urate crystals aspirated from the tophaceous bullous lesion (arrow indicates polarity of light).
Among the acute manifestations, a gouty cellulitis is often seen overlying the massive inflammatory cascade within the synovium of an affected joint. Rarely have bullous gouty lesions been described. Of those that have been documented, the occurrence appears to follow a traumatic episode, similar to patterns described in chronic tophus formation.4 Other acute cutaneous tophaceous reactions, such as the abrupt development of multiple small, inflammatory, pustular gouty skin lesions, appear to be more common and have been described in several case reports.
These reactions, referred to as intraepidermal MSU deposition, have been analyzed in case series, demonstrating an average serum uric acid level of 9.59–11.4 mg/dL.5,6 A review of the handful of case reports of larger inflammatory bullous lesions, dating back to the early 1970s, shows that this is a consistent characteristic of these rare cutaneous manifestations.
